Selective Internal Radiation Therapy (SIRT) für die Therapie nicht resektabler Lebertumoren
|
|
|
- Eva Heidrich
- vor 8 Jahren
- Abrufe
Transkript
1 Selective Internal Radiation Therapy (SIRT) für die Therapie nicht resektabler Lebertumoren Stefan Dresel HELIOS Klinikum Berlin-Buch Klinik für Nuklearmedizin

2 Konzept der SIRT Form der Bestrahlung mit Erreichen einer hohen Dosis an den Tumorzellen unter Schonung des umgebenden Gewebes Infusion über A. hepatica, damit Nutzung der speziellen Durchblutungssituation der Leber 90Yttrium-markierte Mikrosphären (SIR-Spheres ) - Durchmesser ungefähr 30 µm - HWZ: 64 h - Beta 0.93 MeV - Mittlere Eindringtiefe 2.5 mm in Gewebe; max 11 mm - Erreicht HD von 100 1,000+ Gy im Tumor
 - Durchmesser ungefähr 30 µm - HWZ: 64 h - Beta 0.")
3 Leber Toleranz und Tumor Strahlensensibilität SIRT RILD Radiation-Induced Liver Disease Gy: Effektive Dosis: Hodentumoren Lymphome Myelom Kurative Dosen: Adenocarcinome Präoperative Radiatio: Rectum Ca Kennedy et al. Int J Rad Oncol Biol Phys 2004; 60:

4 Verteilung der SIR-Spheres Microsphären in präkapillären Gefäßen

5 Micro-Dosimetrie in explantierten Lebern Monte Carlo Dose Kernel Kennedy et al. Int J Rad Oncol Biol Phys 2004; 60:

6 Wann kann die SIRT angewendet werden? EU Zulassung für die Behandlung nicht-resektabler Lebertumoren Loco-regionale Therapie ohne extra-hepatische Wirkung Anwendbar - in Kombination mit systemischer Chemotherapie für mcrc (1st-line, 2nd-line etc) in Studien für mnet und Pankreasca. (1st-line, 2nd-line) - Als Monotherapie für mcrc und andere metastasierte Tumoren (salvage in chemo-refractory) HCC (1st-line, 2nd-line) mnet (1st-line, 2nd-line etc) Cholangiokarzinom (2nd-line etc) Frühere Anwendung verspricht bessere Wirkung Down-staging vor Resektion oder Ablation möglich
 - Als Monotherapie für mcrc und andere metastasierte Tumoren (salvage in chemo-refractory) HCC (1st-line, 2nd-line) mnet")
7 Einschlusskriterien für SIRT/Radioembolisation Nicht-resektable Leber-dominante oder Leberausschließliche Tumoren Lebenserwartung >12 Wochen ECOG performance status 0 2 Kennedy et al. Int J Radiat Oncol Biol Phys 2007;68:13 23.

8 Ausschlusskriterien für SIRT/Radioembolisation Leberversagen [absolute KI] Schwangerschaft [absolute KI] Vorherige Strahlentherapie der Leber Exzessive Tumor Last mit limitierter Leberreserve Verschlossene Pfortader (nicht, wenn selektives/superselektives Vorgehen) Capecitabine in den vorangehenden oder folgenden 2 Monaten Abnormale Organ- oder Knochenmarkfunktion: - Gesamtbilirubin >2.0 mg/dl (>34 μmol/l) Serum Albumin <3.0 g/dl AST (SGOT)/ALT (SGPT) >5 x Obergrenze Kreatinin >2.5 mg/dl Thrombozyten <60,000/μL; Leukozyten<2,500/μL; Neutrophile <1,500/μL Nach Vorbereitungs-Untersuchungen: Dosimetrie ergibt >30 Gy Lungen-Herddosis [absolute KI] GI Shunt, der nicht behoben werden kann [absolute KI] Kennedy et al. Int J Radiat Oncol Biol Phys 2007;68:13 23.

9 Überblick über die SIRT Prozedur Typischerweise 2-zeitiges Vorgehen Vorbereitung: - Trans-femoraler Katheter bis zur A. hepatica und Identifizierung der den Tumor versorgenden Arterien - Prophylaktische Occlusion extra-hepatischer Gefäßversorgungen - Injektion von 99mTc-MAA/Szintigraphie zur Abschätzung des Lungenshunts Therapie: Wochen später Überprüfung der Occlusion Injektion der SIR-Microspheres Szintigraphische Überprüfung Selektives Lappenvorgehen möglich

10 Tumorboard Onkologie Strahlentherapie Chirurgie Nuklearmedizin Radiologie Konsensentscheidung 1 2 Wochen Tumordarstellung Abdomen PET/CT, CT, MR Leber-assoziierte Erkrankung Screening Untersuchungen Vor Behandlung 1 2 Wochen Bildgebung, Festlegung der Aktivitätsmenge und der optimalen Katheter Positionierung Gefäßdarstellung Leberangiographie, Embolisation extra-hepatischer Gefäße und 99mTc-MAA scan Sichere Applikation möglich 1 Woche Applikation der 90Y-microspheres gleicher Tag Bremsstrahlungs-Szintigramm Kennedy A et al. Int J Radiat Oncol Biol Phys 2007; 68:

11 Überblick über die SIRT Prozedur HELIOS Klinikum Berlin-Buch Klinik für Nuklearmedizin

12 Vorbereitung SIRT Leber-Lungen-Shunt = 29% HELIOS Klinikum Berlin-Buch Klinik für Nuklearmedizin

13 Nebenwirkungen NW Fieber Schmerzen Übelkeit Inzidenz Characteristica Maßnahme >50% mild bis zu einer Woche symptomatisch ~50% ~10% Grad 3 4 mit Applikation verschwindet <24 h Schmerzmittel ~40% innerhalb von 24 h Antiemetika <5% Grad 3 4 Müdigkeit ~40% <5% Grad 3 4 beginnt im ersten Monat post-sirt, dauert bis zu 2 Wochen Abnormale Laborwerte ~20 40% bes. in Kombination 1 6% Grad3 4 mit Chemo-Tx, HCC/Zirrhose; vorübergehend für Tage (ALAT, ASAT), Wochen (Bilirubin) oder Monate (Albumin) adäquate Ernährung prophylaktische Steroidgabe keine
, Wochen (Bilirubin) oder Monate (Albumin)")
14 Komplikationen NW Inzidenz Characteristica Maßnahmen ~5 10% 1 2% grade 3 4 Fehlabfluss; sofortiger, starker Schmerz exakte Vorbereitung, Verschluss GI Arterien, PPI für 1 Monat Pankreatitis <1% Fehlabfluss; sofortiger, starker Schmerz Cholecystitis <1% Fehlabfluss; Schmerz rechter OB RILD: RadiationInduced Liver Disease <1% Gastritis Pneumonitis bislang nicht aufgetreten exakte Vorbereitung Verschluss der GI Arterien symptomatisch Cholezystektomie übermäßige Bestrahlung der Leber; korrekte Beginn d post-sirt; Dosimetrie (BSA); ggf erhöhte Leberwerte, portale Dosis Reduktion Hypertension übermäßige Bestrahlung der Lunge bei Shunt Lungen-Shunt-Best.; <30 Gy Lg.dosis planen
; ggf erhöhte Leberwerte, portale Dosis Reduktion Hypertension übermäßige Bestrahlung der Lunge bei Shunt Lungen-Shunt-Best.; <30 Gy Lg.")
15 SIRT F-18 FDG HELIOS Klinikum Berlin-Buch Y-90 PET Y-90 Bremsstrahlung Klinik für Nuklearmedizin

16 Überblick über klinische Ergebnisse und Erfahrungen bei HCC

17 SIR-Spheres microspheres in Advanced HCC: Survival Median Survival 1.0 SIR-Spheres microspheres Actuarial Survival Control group: months 8 months P = supportive care only P = active treatment P = Months after Diagnosis D'Avola et al. 2nd ILCA meeting 2008; Abs. P-139.

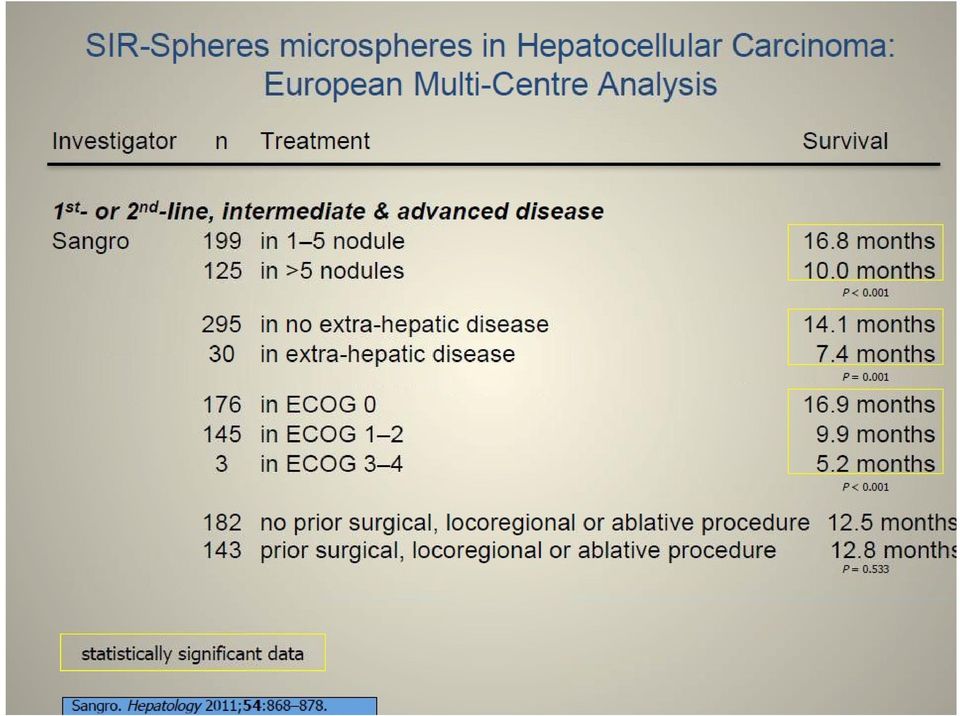
18 SIR-Spheres microspheres in Hepatocellular Carcinoma: Western studies Investigator n Treatment 1st-line, advanced disease D Avola 35 SIR-Spheres 43 standard careδ 1st- or Sangro ORR SD TTP/PFS Survival nr nr nr nr nr nr 16 months 8 months P < >2nd-line 325 SIR-Spheres nr nr nr 52 in BCLC A (unresectable, non-ablatable) 87 in BCLC B 183 in BCLC C 3 in BCLC D 12.8 months 24.4 months 16.9 months 10.0 months 5.2 months P < in Child A in Child B 14.9 months 10.3 months P = Iñarrairaegui 72 SIR-Spheres 14% 80% nr 13 months D Avola et al. Hepato-Gastroenterology 2009;56: Sangro et al. Hepatology 2011;54: Iñarrairaegui et al. Int J Radiat Oncol Biol Phys 2010;77: HELIOS Klinikum Berlin-Buch Klinik für Nuklearmedizin 504-EA-0312

19
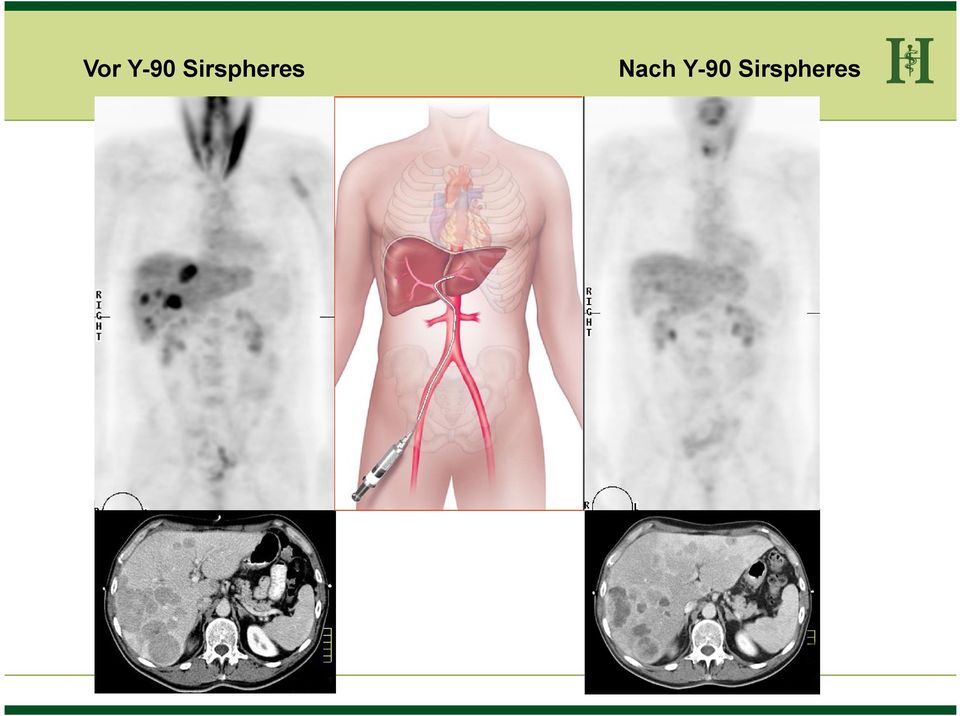
20 Vor Y-90 Sirspheres Nach Y-90 Sirspheres
21 SIR-Spheres microspheres: CT Response Patient 3: Baseline CT scan pre-sirt CT 6 Monate post-sirt; danach Resektion Sharma et al. WCGIC Ann Oncol 2006;17(Sup 6):vi78 Abs P-191..
22 SIR-Spheres microspheres: CT Response Patient 2: Baseline CT scan pre-sirt CT 6 Monate post-sirt Sharma et al. WCGIC Ann Oncol 2006;17(Sup 6):vi78 Abs P-191.
23
24 SIRTACE-Studie Single-session SIRT appeared to be as safe and had a similar impact on HRQoL as multiple sessions of TACE, suggesting that SIRT might be an alternative option for patients eligible for TACE Kolligs FT et al., Liver Int. 2014
25 oligo-nodulär multi-nodulär superselektiv DEB-TACE unselektiv ctace Radioembolisation
26 Behandlung HCC HCC Vorstellung Tumorboard Standard-Kriterien erfüllt? ja nein Leberfunktion und Allgemeinzustand ausreichend? Singulärer Herd oder bis zu 3 Herde Multinodulärer Tumor 1-3 Tumoren 3-5 cm Superselektiver Zugang, keine Pfortaderthrombose 1-3 Tumoren < 3 cm LTX Resektion oder RFA Resektion oder TACE + RFA Kurative Therapie HELIOS Klinikum Berlin-Buch Tumor > 5 cm Resektion ja nein TACE SIRT Transarterielle Therapie Fortgeschrittene Tumorerkrankung, Metastasen, keine transarterielle Therapie Sorafenib Systemische Therapie Klinik für Nuklearmedizin
27 The SORAMIC Study Can the overall survival of patients with HCC be improved by combining sorafenib with RFA or SIR-Spheres microspheres? Design: Prospective open-label, multi-centre, multi-national (Europe) RCT Imaging sub-study Eligible Patients: Unresectable HCC BCLC stage A, B or C Child-Pugh class B7 Fit for sorafenib and micro- <4 tumours <5 cm each Contrastenhanced CT Assign to study arm Primovist enhanced MRI therapy using RFA or SIRT Off Study BCLC stage 0 BCLC stage D Primary endpoints: Imaging sub-study: Non-inferiority (1st step) or superiority (2nd step) of Primovist-enhanced MRI Local ablation: Time-to-recurrence Palliative: Overall survival Sponsor: University of Magdeburg PIs: Prof. Peter Malfertheiner; Prof. Jens Ricke Status: Currently enrolling RFA Randomise 1:1 n = 290 sorafenib placebo local ablation group palliative group Randomise 11:10 n = 375 SIR-Spheres sorafenib sorafenib Secondary endpoints: ٠ Quality of life ٠ Biomarker analysis Imaging sub-study: ٠ Detected lesions and diagnostic confidence Local ablation group: ٠ Detection of recurrence ٠ Safety and toxicity Palliative group: ٠ Safety and toxicity ٠ Overall survival for patients with or without PVT SIR-Spheres microspheres
28 The SARAH Study To determine whether radioembolisation with SIR-Spheres microspheres is more effective on overall survival in advanced HCC than sorafenib Design: Prospective open-label, multi-centre, national (France) RCT Eligible Patients: Unresectable HCC BCLC stage C or BCLC stage A/B: Stratify sorafenib ECOG performance New lesions post-radical therapy and unsuitable for further radical therapy or No objective response after 2 TACE sessions Child-Pugh class A or B 7 points ECOG performance status 0 1 Fit for sorafenib and SIRT status Vascular invasion Prior TACE Institution Primary endpoint: Overall survival Sponsor: Assistance Publique Hôpitaux de Paris (AP-HP) PI: Prof. Valérie Vilgrain Status: Currently enrolling SIR-Spheres microspheres Randomise 1:1 n = 400 Secondary endpoints: SIR-Spheres ٠ ٠ ٠ ٠ Safety and toxicity Quality of life Healthcare costs Progression-free survival (PFS) at 6 months
29 Zusammenfassung Die Anwendung von Sirspheres ist ein sicheres und effektives Verfahren bei hepatischer Metastasierung und primärem Leberzellkarzinom Die Indikationsstellung muss in einem interdisziplinären Tumorboard erfolgen Die Durchführung erfordert die enge Kooperation der beteiligten Fachdisziplinen Die Therapie kann in ein multimodales Therapiekonzept mit anderen Therapeutika eingebunden werden
30 HELIOS Klinikum Berlin-Buch Klinik für Nuklearmedizin
31 SIR-Spheres microspheres in Hepatocellular Carcinoma: Western studies Investigator n Treatment ORR SD 1st- or 2nd-line, BCLC stage C / advanced disease Sangro 24 SIR-Spheres 24% 64% Iñarrairaegui 25 SIR-Spheres branch/main PVT [ 67% ] Sangro SIR-Spheres nr patent portal vein branch PVT main PVT nr TTP/PFS Survival nr 7 months nr 10 months nr 9.3 months 10.8 months 9.7 months P = P = Patent/Branch PVT vs. Main PVT 155 no EHD 28 EHD 10.2 months 7.4 months 37 ECOG ps ECOG ps 1 37 ECOG ps months 10.0 months 10.8 months P = P = Sangro et al. Int J Radiat Oncol Biol Phys 2006;66: Iñarrairaegui et al. J Vasc Interv Radiol 2010;21: Sangro et al. EASL, J Hepatol 2011; Abs HELIOS Klinikum Berlin-Buch Klinik für Nuklearmedizin
32 Integration of SIRT in the HCC BCLC Staging Classification and Treatment Schedule HCC PS 0 Child A PS 0 2 Child A B PS >2 Child C Stage 0 Very Early Stage Stage A Early Stage Stage B Intermediate Stage Stage C Advanced Stage Stage D End Stage single <2 cm or carcinoma in situ single nodule or 3 nodules <3 cm PS 0 multinodular; PS 0 portal vein invasion, N1 M1 or PS 1 2 PS >2 or Child C portal pressure; bilirubin normal Resection single 3 nodules <3 cm increased associated diseases no unilobar fewer nodules smaller burden failed TACE yes Liver Transplant Ablation Curative Treatments 5-yr survival 40 70% 30% of patients bilobar multinodular larger burden TACE SIRT OS 20 months (14-45) 20% of patients (unless within transplant criteria) fit/suitable fit/suitable for SIRT i.e. for sorafenib liver-dominant; i.e. bilirubin main PVT <2 mg/dl; EHD Child A or <B7 SIRT/ sorafenib sorafenib OS 11 months (6-14) 40% of patients symptomatic OS <3 mo 10% of patients Andreana L, Isgrò G, Marelli L et al. Treatment of hepatocellular carcinoma (HCC) by intra-arterial infusion of radio-emitter compounds: Trans-arterial radio-embolisation of HCC. Cancer Treat Rev 2011; 38: Sangro B, Salem R, Kennedy A et al. Radioembolization for hepatocellular carcinoma: a review of the evidence and treatment recommendations. Am J Clin Oncol 2011; 34: